
How Congo’s latest Ebola outbreak unfolded — and why it took so long to detect
The latest Ebola outbreak is the 17th to hit the Democratic Republic of Congo (DRC) since the virus was discovered in 1976. It is already the fourth-largest outbreak in history, according to data from the World Health Organization (WHO) and Centers for Disease Control and Prevention (CDC).
Global health experts have been quick to criticize what they describe as a slow and fragmented response to the outbreak, pointing to recent cuts to global health programs under the Trump administration, including the withdrawal of support for the WHO, the dismantling of the United States Agency for International Development (USAID) and reductions to several global health funding streams.
However, it remains unclear to what extent those policy changes have directly affected the response to the current Ebola outbreak, due in part to limited transparency from the Department of Health and Human Services (HHS) and the State Department (DOS) about how their infectious disease surveillance, prevention and response operations are currently functioning.
Straight Arrow spoke with former federal disease-response officials, frontline health workers and public health experts, reviewed years of epidemiological and outbreak-response data, and contacted multiple U.S. government agencies and officials — many of whom declined to answer specific questions — to piece together how the outbreak unfolded and how the response has been shaped by recent changes to global health infrastructure. What emerged was a portrait of an outbreak response slowed by local instability, a rare and difficult-to-detect Ebola species and lingering questions about how recent changes to U.S. global health infrastructure may have affected surveillance and response efforts.
What we know about the Ebola outbreak timeline
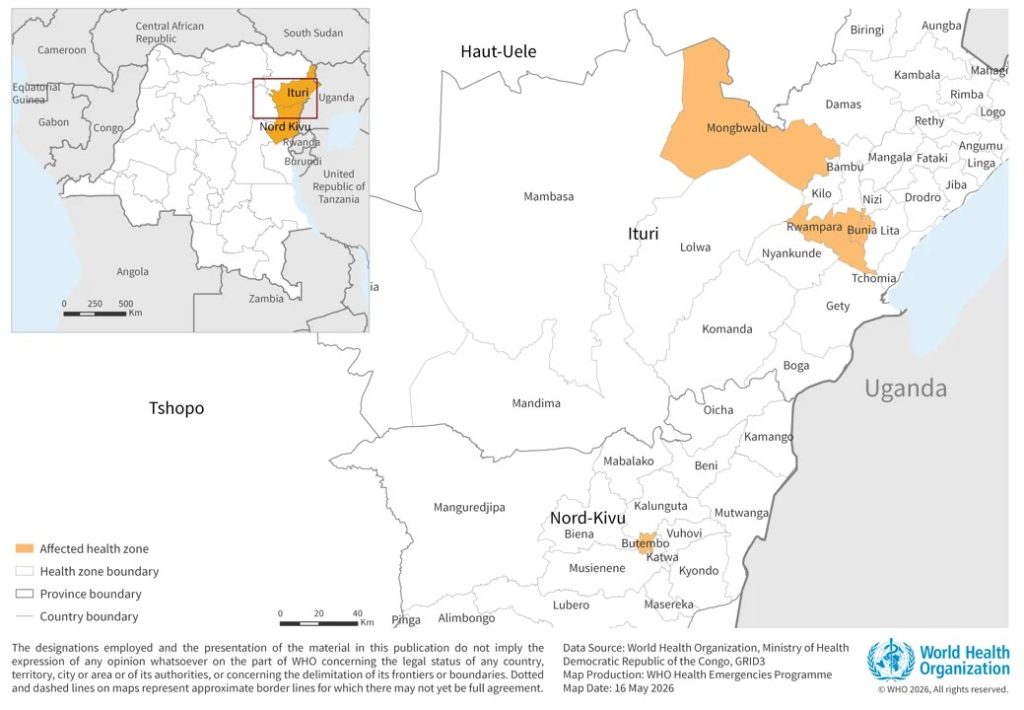
On April 24, a 59-year-old man suffering severe symptoms of an unknown disease sought treatment at a hospital in Ituri Province, in the northeastern corner of the DRC. That same day, a nurse in the region also fell ill and sought out medical care.
The two patients are believed to be among the earliest known cases linked to the latest Ebola outbreak in the DRC, though investigations are ongoing and additional earlier cases may still be identified.
At the time, neither their doctors nor health officials knew they were dealing with Ebola. Both patients later died.
In the following days, more people arrived at clinics and hospitals across the region with a severe and unexplained illness. Some of the healthcare workers caring for them also became sick. By May 5, when Congolese health officials alerted WHO to a cluster of unexplained deaths in Ituri Province, at least 50 people — including four healthcare workers — had already died, according to the Africa Centres for Disease Control and Prevention (Africa CDC).
On May 13, authorities dispatched rapid response teams to investigate. Two days later, laboratory testing confirmed the worst: A rare type of Ebola known as Bundibugyo virus was spreading through northeastern DRC.
By the time officials publicly declared an outbreak on May 15, Congolese health authorities were tracking 246 suspected cases and 80 deaths. And the virus had already crossed international borders.
In neighboring Uganda, a laboratory test confirmed that an elderly man who died after traveling to the DRC was infected with Bundibugyo. Later that week, Ugandan officials confirmed a second imported case in Kampala involving another traveler returning from the DRC who appeared to have no connection to the first patient.
‘Our surveillance system failed’
If the late-April cases are truly the first of the outbreak, then it took local healthcare workers and public health officials 11 days to report the unusual pattern of cases to the WHO and 21 days to identify that the Ebola virus was behind the cases and to declare an outbreak. The response time was slower than previous outbreaks.
Late last year, officials declared the country’s 16th Ebola outbreak, just 12 days after health workers encountered what was believed to be the first case. Between February 2021 and July 2022, the Ministry of Health declared three additional Ebola outbreaks, 13, seven and 18 days, respectively, after the first known patients arrived at local hospitals. Those outbreaks occurred as U.S. government spending on global health peaked and as the Biden administration surged funding to help countries respond to the COVID-19 pandemic.
Earlier outbreaks often took significantly longer to identify.

In 2014, as West Africa struggled through the deadliest Ebola epidemic in history, officials in the DRC were simultaneously working to contain a separate outbreak within the country. It took authorities 29 days after the first known patient developed symptoms to recognize that Ebola was spreading. During three other outbreaks between May 2018 and November 2020, officials waited more than a month after the earliest known patient became ill before formally declaring the outbreaks.
It remains unclear why it took so long for health authorities to recognize and report the growing cluster of unexplained illnesses and deaths. But local public health experts said the delay suggests that the region’s disease surveillance and reporting systems did not function as intended.
“Our surveillance system failed,” Jean-Jacques Muyembe, director-general of Congo’s National Institute of Biomedical Research, told Congolese reporters Sunday.
Editor’s note: Jean-Jacques Muyembe’s remarks have been translated from French.
Muyembe attributed the delay in laboratory confirmation to a lack of appropriate diagnostic testing in the region. The tests available to laboratory technicians were designed to detect only the Zaire species of Ebola — the most common and deadliest form of the virus — and were not capable of identifying Bundibugyo. Bundibugyo virus is among the rarest known forms of Ebola and has caused only three documented outbreaks since it was first identified in 2007.
By contrast, the Zaire type has caused at least 28 outbreaks and carries an average fatality rate of nearly 70%, according to a review of CDC and WHO historical outbreak data. Sudan virus, the second most common Ebola species, has caused nine known outbreaks worldwide and has historically killed about half of those infected.
In the two previous Bundibugyo outbreaks, case fatality rates ranged from roughly 32% to 34%. In the current outbreak, 131 people have died among 513 suspected cases, DRC Health Minister Samual Roger Kamba said Tuesday, suggesting a preliminary fatality rate of about 25%. However, that figure could change as investigators identify additional cases and deaths and confirm which suspected infections were caused by Ebola.
Although effective vaccines and treatments exist for Zaire ebolavirus, there are currently no approved vaccines or therapies specifically for Bundibugyo virus.
Muyembe also said frontline healthcare workers should not shoulder all the blame for the delayed detection of the outbreak, arguing that monitoring infectious disease outbreaks is a broader societal and political responsibility.
“Monitoring an epidemic isn’t just the Ministry of Health’s responsibility. It’s everyone’s responsibility,” he said. “In this region, you have members of parliament and senators who go on vacation and are aware of the situation. They know there are deaths, and nothing is said.”

The outbreak’s location may also have led to delays and hampered future response efforts. Ituri Province has long been one of the most volatile regions in eastern DRC. Years of armed conflict, intercommunal violence and other disease outbreaks have displaced nearly 1 million people and left more than 2 million in need of humanitarian assistance, according to Erica Tavares, the senior director at International Medical Corps, a global nonprofit that is helping to respond to the outbreak. The prolonged instability, alongside poor infrastructure, has repeatedly disrupted humanitarian operations and made it difficult for health workers to safely monitor and respond to disease outbreaks in the region. Moving people and medical supplies into and around Ituri Province will also be a challenge, she said.
“It’s a very hard operating environment, and I wouldn’t assume that even if the surveillance capacity was perfectly intact, even if the lab capacity was intact, even if commodities can get in country, it would still not be easy to respond to this outbreak,” a former senior USAID leader who helped lead the agency’s response to previous Ebola outbreaks, told Straight Arrow. The former staffer asked to speak on condition of anonymity.
“The other possibility is that the government was not forthcoming in sharing information. But from the engagement I’ve had with the DRC government over the last several years, I don’t think that is likely the case, because they’ve actually really improved in transparency and information sharing,” the former USAID staffer said. “My sense is that they’re probably stretched quite thin, doing a lot at the Ministry of Health with less funding resources, given the funding cuts, in particular.”

Are Trump administration funding cuts hindering Ebola response efforts?
Looming over the response is the gap left by the Trump administration’s retreat from global health and foreign assistance programs, which some public health experts fear may have weakened the surveillance and response systems designed to detect outbreaks before they spiral out of control.
Historically, USAID and CDC coordinated closely in the DRC and other countries. The CDC focused on providing technical support to improve disease surveillance, laboratory capacity and outbreak detection. USAID supported logistics, supply distribution and community engagement efforts critical to controlling Ebola transmission, including promoting safe burial practices.
But the Trump administration has scaled back global health and foreign assistance programs.

Last year, the administration shuttered USAID and terminated many of the agency’s contracts, though some programs were later transferred to the DOS. The full extent to which Ebola-related and global health programs survived the transition remains unclear. The DOS did not respond to Straight Arrow’s inquiries.
The CDC also underwent significant staffing reductions. More than 1,300 employees were initially notified that their positions were being eliminated, but the agency later reinstated roughly 700 of those roles. It remains unclear whether the staffing changes affected CDC country offices in the DRC or Uganda.
Around the same time, the Department of Government Efficiency (DOGE) reportedly canceled several Ebola-related contracts that funded airport and border disease screening, supplied protective equipment for healthcare workers and supported programs aimed at preventing Ebola survivors from spreading the virus. In February 2025, Elon Musk, then the leader of DOGE, told Cabinet officials that the administration had “restored the Ebola prevention immediately, and there was no interruption.” However, USAID officials at the time said airport screening operations had been paused for at least two weeks.

HHS spokesperson Andrew Nixon did not answer Straight Arrow’s specific questions about CDC staffing. He did say, “CDC maintains extensive expertise in viral hemorrhagic fevers. CDC is fully equipped to protect Americans and mitigate risks through experts in this disease area.”
President Donald Trump also withdrew the U.S. — historically the largest donor — from the WHO, triggering major budget shortfalls, hiring freezes and thousands of staff cuts. WHO Director-General Tedros Adhanom Ghebreyesus warned the move would weaken global disease surveillance and emergency response efforts, saying the withdrawal would make “both the United States and the world less safe.”
The U.S. is not the only country to cut funding for global disease prevention, outbreak response and humanitarian aid. The U.K. reduced its foreign aid budget from 0.7% of gross national income to 0.5% with plans to further reduce that to 0.3% by 2027. Other major donors, including Germany, Japan and France, have also slashed global health and aid budgets in recent years.
How is the US involved in the Ebola response?
The State Department announced Monday it had allocated $13 million in foreign assistance funding to support the Ebola response. Additional bilateral funding for outbreak response and humanitarian assistance could be announced, the department said, as officials gather more information about the scale of the crisis. U.S. government spokespersons also said additional personnel were being mobilized to the region, though officials did not specify how many staff were being deployed or what types of specialists were being sent.
Despite broader concerns about cuts to global health programs, some aid groups working on the ground say the U.S. government moved quickly to support the immediate outbreak response.
”The Department of State has been on top of it. They’ve certainly partnered with us, and I know other partners as well, and were there and looking to stop this outbreak,” Tavares told Straight Arrow. “From that perspective, they’ve been the same kind of partner that we’ve worked with for the last 40 years.”
During a press conference Monday, officials said the CDC was working to bring home a small group of Americans “directly affected” by the outbreak. At least one American, physician Peter Stafford, has been infected with Ebola.
The public health agency also announced it was invoking a Title 42 order barring non-U.S. citizens from entering the country for 30 days if they had traveled to the DRC, Uganda or neighboring South Sudan within the previous three weeks.
HHS spokesperson Nixon told Straight Arrow that the CDC is “working with international partners and Ministries of Health on this evolving situation and is supporting response efforts through its country offices in the DRC and Uganda.”
“This support includes technical assistance with disease tracking and contact tracing, laboratory sample collection and virus sequencing, infection prevention and control, local border screening, coordination with affected countries and international public health partners, distribution of personal protective equipment and infection control supplies, and risk communication and community engagement in affected areas,” Nixon said.
HHS did not respond to requests for more specific information and did not permit Straight Arrow to interview CDC experts.
Round out your reading
- They built an Epstein files library, but realized they couldn’t let everyone read them.
- The doctor who claims functional medicine reversed her MS.
- For many Americans, ‘one more round’ no longer serves their lifestyle or budget.
- Trump claimed economic data is ‘rigged.’ Former officials pledge to ‘watch like hawks’ for political manipulation.
- We’re building a new Straight Arrow. Help us shape our future by taking our survey.




